What the Affordable Care Act Means for Physician Assistants
Posted By: Paul | The Basics | 29 Comments
“Obamacare” is now a reality. Last week’s US Supreme Court Ruling has huge implications for the future of our nation, and even bigger implications for the physician assistant profession. In this article I’ll give you the Cliff Notes version of the new law, why it came about, and what it means for the you. If you already understand the new health care reform, you can jump to my predictions for the profession below.
A Thumbnail Sketch of the Health Care Crisis
First, the big picture.
- For years the cost of health care has been increasing much faster than anyone’s ability to pay for it, including the government. Ten years ago, the federal government spent 17% of its budget on health care. This year, it’s up to 22%. At its current rate, by the end of the decade it will hit 25%. Most economists agree that this pace of growth is unsustainable. Where does it all go? Uncle Sam spends this money primarily on two programs: Medicare (a health care program for all adults over 65, and others who are permanently disabled), and Medicaid (a health care program for those who have limited income and resources).
- Employers are similarly unable to keep up with the cost of insuring their employees. Health care costs have caused the failure of many small businesses that can’t bargain effectively for lower rates.
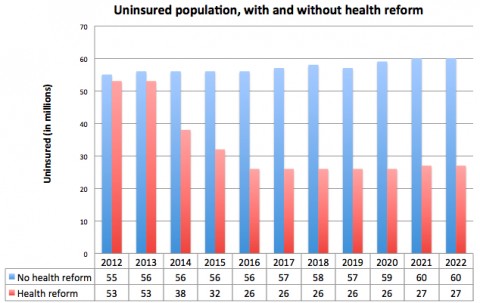
- Rising costs left approximately 50 million Americans without health insurance this year.
- Health insurers have been unable/unwilling to allow coverage for those with pre-existing conditions, because these people are sicker and therefore more expensive to insure. This has reduced competition that is needed to help control costs.
{kind=link}
What is the Affordable Care Act (ACA)?
- In an effort to reduce the financial burden on the federal government, the Obama administration introduced the Patient Protection and Affordable Care Act. The ACA was a sweeping health care reform bill that was signed into law by President Obama on March 23, 2010 and upheld by the US Supreme Court’s landmark 5-4 ruling on June 28, 2012. The high court ruled that most of the ACA’s provisions are constitutional and therefore may be implemented.
- The largest and most important provision of the act is the so-called “individual mandate,” which will effectively require all Americans to purchase health insurance by taxing those who do not do so by the 2014 deadline. The individual mandate was intended to bring healthy citizens into health care so that their relatively inexpensive health care needs could help to compensate for the more expensive care of those who are older, or who have pre-existing conditions.
- The end result of the individual mandate is that an estimated 32 million Americans who have no health insurance will get it.
- The federal government will subsidize insurance for those who cannot afford health insurance for the time being.
- There are many other provisions of the law, including the expansion of Medicaid, the establishment of insurance exchanges where consumers can “shop” for health insurance, prevention of insurance companies from dropping patient coverage capriciously, and payment for preventive medical care.
How Will The ACA Affect the Physician Assistant Profession?
The ACA will significantly increase the number of Americans who have health care - this represents a major expansion of the health care industry. No one is sure yet how all of these 32 million new patients will be cared for. If you’ve gone for a check up lately, you’ve seen how busy doctors are already.
Projection #1: The already huge demand for PAs will increase dramatically.
Why? Doctors cannot fill this provider gap. But, you might wonder, “Can’t they churn out more doctors by opening more medical schools, just as they are doing with PAs?”
In a word, no.
The shortage of doctors isn’t about not having enough medical schools. It has to do with a different bottleneck. What limits the speed of doctor training is the residencies that they are required to complete after medical school. Ironically, the money that funds residencies comes from Medicare - one of the already financially troubled programs that the federal government is working on with this law. For this reason, no one expects much increase in the number of doctors in the coming decade.
Physician assistants, on the other hand, do not do residencies. They graduate from PA school and go to straight to work. Their education is far less expensive. Although there is a nearly 20-year-long projected shortage of physician assistants, the rate at which new PAs are being licensed is increasing annually, as new PA programs are established. Even better, the new health care reform law provides money for new physician assistant training programs. The end result? PAs are in a much better position than doctors to fill the health care gap.
Projection #2: More than ever, PAs will be needed for primary care and pediatrics
When you speak of preventive health care - things like vaccinations and annual check ups which under the new law will now be covered - you’re talking about primary care and pediatrics. For the profession as a whole, this is good news. All PAs are trained as generalists, even if they end up specializing after their schooling. But if you were hoping to work in a specialty such as ophthalmology or surgery, this news might not benefit you much. Specialists will still be needed. But supply and demand may begin to improve the salary of those in primary care, and this could mean slowing of the salary increases for those in specialties. One of the aims of the reform is to reduce the overall amount of expensive (and sometimes unnecessary) specialist care by replacing as much of it as possible with primary care. But if your heart is set on a particular specialty, don’t panic; equalizing primary care and specialist pay could take a long time, if it happens at all.
Projection #3: There will be less need for PAs in specialties like cardiology, pulmonology, and endocrinology.
These are specialties that in addition to providing specialist care, often provide primary care as well. If you have severe emphysema, for example, it sometimes makes sense to have a pulmonologist provide your general medical care, since most of your visits are likely relate to your lung disease. But with more primary care and preventive care being delivered and increased scrutiny about what problems are sent to specialists, this practice will become less common. There are likely to be fewer patient visits to see these specialists, and therefore less demand for PAs in these areas.
Projection #4: More than ever, PAs will be needed in mental health.
Traditionally, insurance coverage for mental health care has lagged far behind that of illnesses like diabetes and high blood pressure, but that is likely to change. Recently passed “parity” laws make mental health conditions equivalent to those that have been traditionally considered more “medical,” and they will be paid for equivalently as well. Not only will mental health be treated more like a physical illness, most of those with mental illnesses will finally have health insurance. If you have an interest in psychiatry, the world will be your oyster.
Projection #5: Emergency medicine will change for the better and the worse.
With a new emphasis on primary and preventive care, and growth in health care overall, there will be fewer ER visits from patients who need help with chronic conditions like arthritis and allergies. These patients will still have chronic health problems, but they will have better access to resources that are more appropriate than the emergency room. If you work in the ER or plan to, this probably sounds great. But what isn’t so clear is how these changes might affect the overall number of ER visits per year, and therefore the demand for Emergency Medicine PAs. The new law eliminates some of the penalties for patients going to out-of-network emergency rooms, and generally makes ER access easier. But again, the hope is for fewer visits from patients with non-emergent conditions. The hope is that emergency care might slowly return to its original purpose: preventing death and disability, and not its too-frequent one: 24/7 pharmacy and outpatient care.
Why Do You Need To Know This?
Even if health care policy and politics doesn’t interest you much, you would do well to learn about it. This is great material for a PA school interview question, and understanding these issues can make your motivation to become a PA more convincing. What’s more, this is going to be your field - the more you know, the more you can influence it.
29 Comments
Comments are closed.
Recent Works



Latest On The Podcast

This is a great article and is very important to PA’s and future PA’s. With the changing healthcare landscape and the aging/growing population the role of PA’s will become ever more instrumental in healthcare. I agree with your assertion of the increasing demand for Physician Assistant’s especially in primary care. I am very happy about the greater recognition of mental health as an illness, and more practically I am very happy about the future insurance coverage of these illnesses. However I still believe that the role of PA’s will be very important as primary care providers for, especially for patients with type II diabetes and diabetes related diseases. Diabetes has been a growing national and global concern that has become even more important in light of current evidence showing not only the growing number of diabetics, but the number of prediabetic adults, young adults and adolescents. The following years will be interesting. Thank you for the great article!
P.S. How did the PANCE go?
I’m waiting to hear. I thought it went pretty well, but I’ll feel better when I see that I’ve passed.
Thanks for your interest!
I’m sure you did well. I remember when I took my board exams (ASCP not PANCE), it feels great to be done but the anxiety remains until the results come in!
Ditto TitanEAG!
Thank You! Your posts and articles are MUCH appreciated. Hope PANCE went well!
very informative and im positive you passed
Good article, Paul. Interesting projections. I think it will be a good time to be a PA. But I think that is true now as well.
Looking forward to hearing about your PANCE!
Excellent article. As always, thank you for your time and effort in providing us with helpful information regarding the PA profession and getting into school.
From Clinician1.com
I was watching the various news stations Thursday morning reporting on the soon to be reported decision by the Supreme Court on the Affordable Care Act. Regardless of the outcome, I knew that the politicians would all use the ruling as a sound bite to air on Fox or CNN and that many others would view the decision only through the lens of politics. I was going to head down to a meeting where I would be spending two days interacting with a group of NPs and PAs who would all be affected by this decision (more on that meeting next blog). I began to ask myself, what did this decision mean to the members of Clinician 1 and in a larger scope to the NP and PA professions. Putting my own politics aside, I knew it is a seminal moment for both professions. We will have to bend and change to fit into some of the changes that our medical care system will need. Not just medicine but insurance companies, legal and hospital systems and almost all healthcare professions will be changing.
So if you are a PA or NP what will it mean?
-First and foremost it will give us a greater opportunity to define our professions and their place in the healthcare delivery system of our country than ever before.
We will have an increasing number of patients needing care. Millions and millions of them. If we can deliver that care, all the better. If we can design better systems using NPs and PAs we will hit a number of home runs. If we can’t, physicians will, and my guess would be we will be left out of the decision making. Millions of people are going to need care and every health professional will be figuring out how to be the one that provides that care. Like it or not, there is considerable money to be made in all of this and all kinds of providers and health systems will line up to grab their share.
-Harder work
My guess is whatever your specialty you are in, you will work harder. Patients who are newly covered by insurance will need services, many will need tests they should have had years ago. Some will need surgery. Some will need an appointment to the sleep lab. All will need us to see them.
-More Students
APCs are the professions best positioned to train people quickly and at less cost to the system to provide primary care. Schools, if they have not done it yet, will increase enrollment. More money will flow into PA and NP education. More positions will open and getting into an NP or PA program will continue for many to be a key to a much better future. Competition will also increase as will the demand for good faculty and good preceptors. If you can take a student starting today, please do. If you want to retire soon, teach for a few years first. If you just say “Let the next person do it”, shame on you.
-More of a Primary Care Positioning
Many PAs and NPs have gone into specialties. Although the FNP is the degree choice of the majority of NPs, one little secret in the NP world is many people do not stay in family practice. As PAs have been doing for many years, the NP profession has been attracted by the specialties that pay more. That is fine and that is what America is about, but our two professions will have to re-steer some of those clinicians back into primary care and family practice. As importantly, we will have to steer our new students towards a meaningful career in primary care. The Association of Family Practice PAs (www.afppa.org) has written a wonderful position paper which applies to NPs as much as PAs regarding “The Future of PAs in Primary Care”. Here is the link if you want to read it. http://clinician1.com/posts/article/afppa_statement_the_use_of_pas_in_primary_care_2012/ If you agree, join the organization as they are fighting for you. The statement looks at starting/expanding residencies and using Medicare monies to fund residencies (physician residencies are funded by Medicare funds) to increase the expertise of PAs and NPs in family practice. Especially the new grads. Part of that education must also look at evolving new models of care, teach medical staff supervision and add clinical skills we feel need to be better at.
We need to show that we too can innovate and do it in the context of primary care. This is something the physicians have generally been unable to do.
-Better NP and PA Relations
Unless we want to re-enact the struggles that existed for many years between the MDs and DOs we have to work together whenever possible and resist trying to the the only big winner. Why? Because there are too many people working against us and also because there will be no one “big winner” in this exercise. It has to be win/win and as much as we can we should try to include physicians in that winning equation. Their inclusion, when it does not compromise our values, is the smartest thing we can do. While I do expect organized medicine to oppose much of what PAs and NPs try to do, they will have no better answer than us and the majority of America’s physicians already work with us. We all need to understand each other better.
Better Identity and More Autonomy
As I eluded to, the system needs us all more than ever. PAs should make an attempt to slowly change their professional name to Physician Associate (let’s start with some of the programs) and start re-defining what we do and how we practice. I am sure most PAs would love to insert the word collaboration where it says supervision. For the PAs that feel we will put all we have gained at risk I have two thoughts. If the system needs us so much, will the system allow us to lose anything? Especially those skills that would stop us providing care? I really doubt it. A title redefinition and change should leave no one angry at us if we explain it correctly and go about it with thought. The second is, if we are expected to really contribute, assistant will hold us back. While NPs will be gaining independence, the perception that we “assist” kills us. We can only hold ourselves back by fear of needed change.
It is also clear that we NPs and PAs should stop saying “We do the easy cases, so that we can free up physicians to handle the more complex ones”. It may have worked in the 60s but it won’t work under a re-designed healthcare system where primary care PROVIDERS are needed. While it might be true in many cases that the physicians training allows them to do more (surgery, pathology and other specialties), that is generally not true in day to day primary care. At best it’s misleading as there are no “easy” cases and at worst it says we can only do half the job. We have to start thinking that all of us are well educated and can treat anyone who walks in for care. Those we need to refer, either to a surgeon, a psychiatrist or an NP or PA down the road, we will. Saying we only treat the easy patients cuts both professions short and reinforces what some believe about us. Let’s just say, the system will need us to “Be all that we can be”. PAs are great and so are NPs. Both more than able to provide primary care. Let’s tell people that.
The Affordable Care Act is history. Even if a new President wins, the medical care system will continue to be re-designed.
Let’s seize the moment to make ourselves better providers and work together professionally to decrease the barriers we all face daily.
Dave
Thanks for your thoughts, Dave. I agree with pretty much everything you’ve shared. To add to your point about the importance of collaboration with doctors, the idea of increased autonomy in a field that is designed around PA & doctor teams would really take a hit if we tried to “go it alone.” We need the support of doctors, not their interference. Though we do much care by ourselves, we need them to make sure we are giving the best care that we can.
Love reading your articles! I’m a 4th year PA student, and it’s so nice to have information like this put simply and to the point!
Good luck with your PA career!
Thanks, Stephanie! Spread the word, okay? Thanks!
P
Great summary. I just have one question regarding the lifestyle for PA’s. With the ACA putting more patients into the healthcare system and bringing with it a larger workload for healthcare professionals, will the idea that PA’s have a slightly balanced lifestyle (having time for families, outside interests, etc.) become a thing of the past?
It certainly could. But I hope that the creation of PAs and their proper use will ramp up quickly, so that the demand doesn’t outstrip the supply by loads. But if it does, this could mean better compensation for those who choose to see more patients and do more “hard” types of work, while those who place more value on life balance may be willing to earn less.
Thank you so much Paul. This is a phenomenal site and your insight is great.
Thanks for the article. There is SO much to the ACA that it can be difficult to find SOLID information. I hear people talk about the ACA including a REQUIREMENT that there be one physician for every so many PA’s in the future, but I cannot find any information confirming or dismissing this. Do you have any info regarding that assertion?
I’ve never heard that, and I doubt it is seriously being considered.
That’s what I figured. Thanks!
Hey, Thank you for your insight and research. This is helping me well for my research paper. 🙂
Paul- Great information on this post. I agree with the points that you have made about the effect of the PPACA and midlevel practitioners. I am currently working towards applying for PA school myself- I have been researching, shadowing, and working alongside the profession for about 4 years. I am currently completing my Masters in Public Health- which so far has been a critical (and beneficial) step in my journey to becoming a PA (student). I recommend all midlevels to educate themselves in public health. Many of the points that you have made here are constantly being covered in many of my classes. In all of this I think that collaboration will be key- working together with the doctors/NPs/Nurses/Healthcare Admin could prove effective in providing more accessible high quality care in the communities that we serve. I’m hoping that in the future my public health background will make me a more effective provider, associate, and leader in underserved communities. -Thanks for posting 🙂
A friend of mine who is a fourth year med student was telling me the other day that with the ACA, PAs will take a hit when it comes to acting as 1st Assist in surgery. As of right now, if I’m not mistaken, PAs are reimbursed at around 12-15% for surgeries when acting as 1st assist, but that will decrease (if not completely vanish) with the ACA. I can’t confirm or deny this, but I would like to do more research. Most articles I read are similar to this one and mainly talk about the Pros. Anyone heard more about this?
The ACA is about making care more affordable, and this means using more PAs, not fewer. Currently, having a second doctor assist a first is uncommon, except for those in learning hospitals, where a fellow or resident might assist the lead surgeon.
The vast majority of PAs, particularly surgical ones are paid on salary, not by the surgery, as private physicians are. This means that to take this “hit,” they would need to lower a PAs salary, and these days, that’s unheard of. It could happen, but the trend is very much in the other directly now. The most I could see this ever doing would be to slow the growth of PA salaries, but I still doubt that.
But the truth is, no one really knows what Obamacare/ACA is going to look like yet - we’re all holding our breath.
I’m not really worried about PA pay going down or hurting the field. I was more commenting on reimbursement in general. If a PA is generating a 15% income for the practice for every first assist he/she does on a surgery, the practice itself will be taking a 15% hit if that is taken away. I would say that is a negative aspect of the healthcare reform and how it relates to PAs. You may be paid a salary, but knowing that you are not getting reimbursed for your contribution is a bit of a let down, as well as knowing the practice that you work for (and hopefully enjoy) is not as profitable as it used to be. Working for a hospital or larger organization might be another story.
Either way, it’s just another reason why it is important for PAs to stay informed and active in legislating for our profession.
The story my med student friend told me was of a PA, who even though he was paid salary, was given the 15% he generated as first assist as a bonus at the end of the year. I was told that this added up to around $50,000 or so. Again, I can neither confirm or deny this, and obviously would not be your typical situation as a PA. If this story is true, the PA has a very generous doctor they work for.
All in all, I know the healthcare reform has a LOT of pros for the PA profession. I just think we should be aware of any negative aspects we may run in to.
That’s a very rare occurrence. The vast majority of surgical PAs are paid on salary, which means they get the same whether they perform 3 surgeries per day or 5. The commission-type system you’re talking about is an oddity. But I’m sure there must be some PAs out there who are paid by the surgery. If it makes you feel any better, surgical PAs are paid a handsome salary, so it’s probably just as well that they aren’t paid per procedure.
Excellent article! I had some insight to what the new healthcare reform will do for our nation as a whole, but this gave me even more perspective on how it will affect my future career. Thanks!
As more PA’s become primary care providers, how do you think this will effect their liability?
I think there will be a pull for them to expand their scope of practice, and work even more independently, since the ratio of MDs to PAs seems to be shrinking (because there are more PAs). But the profession continues to lobby for the license to be able to do more, while at the same time lobbying for more protection from malpractice. But PAs will ultimately ALWAYS be under the supervision of a licensed MD.
I am not trying to poo poo on anything that’s been said but is anyone else worried about the dramatic increase in not only PA programs but NP programs? There is at least one NP program in the state of KY that allows them to do it ONLINE! Scary? It should be. By my estimates there are 4 PA programs in the state and 4 NP programs. I have no “true” estimates for how many nurses are doing their online training but I believe yearly in the state all programs combined would be graduating about 800 mid level practitioners. And that is one state. Where will all these practitioners go? Many areas are saturated now. That’s why you get big offers to go to Alaska and Wisconsin. No one is out there. I just wonder if both PA and NP programs are shooting themselves in the foot. Supply and demand can be a bad thing for a profession at times. The ACA is by necessity going to be changed because it is unsustainable. The idea is honorable. Health care to all. But when you get basically “free stuff” do you want more or less “free stuff”? I’ve had Medicaid patients come into the ER 3 times a week for the most minor complaints. That money has to come from somewhere. The Medicaid patients are increasing not decreasing.
Hi, Rob!
I think there are two separate issues here.
1) are there too many PAs (I’m choosing not to speak of NPs — not my area, and a different certificate)?
and
2) Is the ACA sustainable?
There was a HUGE shortage of primary care physicians BEFORE the ACA was passed, so you better believe that there is a GINORMOUS shortage of them now. The US Bureau of Labor Statistics is estimating a shortage of PAs for more than the next 20 years, and that’s with the projected rate of increased programs. I’m not saying PAs have guaranteed employment, but things look pretty bright for them in terms of demand.
As for #2, I have serious questions about the sustainability of the ACA myself. But the money was already “coming from somewhere” before the ACA was passed. There were just as many people going to the ER with stupid complaints back then as there are now. But back then the hospital or the insurance was eating the costs, and now it’s the insured. People who don’t cost a lot are now paying for all the ones who do. BUT few people remember what a mess MediCare was when it was established in 1966. Now it’s a sacred cow in this country. The only reason that it’s in trouble is that politicians have always borrowed from the MediCare trust fund, not because it doesn’t have enough money.
Finally, I think ACA was a necessary step. First give everyone care. Unfortunately, it did nothing to reduce costs. I hope that cost reductions will be the next big step.